Carpal Tunnel Syndrome – All You Need To Know
Carpal Tunnel Syndrome is the most common neuropathy and is due to the compression of the median nerve of the wrist in its passage through the carpal tunnel.
Contents
What is the carpal tunnel?
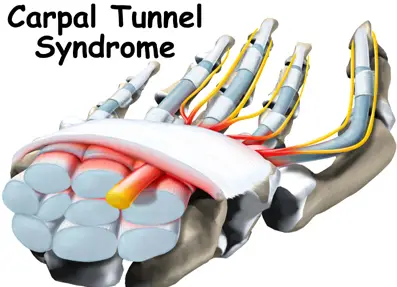
The carpal tunnel is a channel located in the wrist, which is formed by carpal bones upon which the transverse carpal ligament is stretched. The latter is a fibrous tap which makes up the roof of the actual tunnel as it inserts itself upon the scaphoid and trapezius bones on one side and the carpal hand bones (the pyroform and hookbone) on the other side.
Nervous structures (the median nerve) run through this tunnel together with vascular and tendon structures (flexor muscle tendons of the fingers).
What are the causes of the CTS?
Occupational pathogenesis seems to be the most frequent cause of Carpal Tunnel Syndrome development. An association with repetitive tasks, both with (higher risk) and without the application of elevated force have been shown.
It has also been shown that prolonged and/or repetitive wrist flexion/extension movements (to a lesser extent also finger extension) provoke an increase of pressure within the carpal tunnel and that the continuous lengthening of the nerves and muscles in the tunnel can bring about an inflammation which reduces the same tunnel’s dimensions determining compression of the median nerve.
Other systematic illnesses can be associated with Carpal Tunnel Syndrome (e.g.: Mellitus diabetes, rheumatoid arthritis, myxedema, and amyloidosis) so as for physiological situations (pregnancy, use of oral contraceptives, menopause), traumas (wrist fractures with articular deformation), arthritis and deforming arthrosis.
What are the symptoms of CTS?
In the initial stages of the pathology, Carpal Tunnel Syndrome (CTS) manifests itself with pins and needles, numbness or swelling of the hand, mostly to the first three fingers and partly the fourth finger, above all in the morning and/or during the night; successively pain is felt which radiates also to the forearm, these symptoms are defined as “irritating”. If the pathology worsens, loss of feeling in the fingers, loss of strength in the hand and atrophy of the thenar eminence is manifested. These symptoms are defined as “deficitary”.
Which are the jobs more at risk?
Carpal Tunnel Syndrome presents a significative association with some occupational sectors. Those hit more are workers in manufacture sectors, electronics, textiles, food industry, shoes, leather industry and also workers in packing departments, hotel chefs, and workers in Public sectors.
Why are the symptoms prevalent at night and upon waking?
The views on this are not univocal. Actually the causes are many: during the night the wrist may be hyper flexed or hyperextended thus determining, as explained above, a major pressure within the carpal tunnel, with the compression of the median nerve; the lying position may redistribute body liquids with an increase in the higher limbs and therefore within the carpal tunnel with a consequent increase of pressure; The actual resting of the hand does not permit liquid drainage from within the carpal tunnel.
What is the frequency of the Carpal Tunnel Syndrome?
Studies aimed at this aspect do not give univocal results; this is understandable in view of the variables involved (different selection criteria, the job was done, diagnosis criteria, etc.). A study conducted from 1983 to 1985 in Holland shows a rate of 3.4% in women and 0.6% in men, but it is estimated that CTS is present to a further 5.8% in undiagnosed women (De Krom et al. J Clin Epidemiol 1992; 45:373-6). The average annual occurrence calculated during the period 1961-1980 in Minnesota is 149 every 100,000 inhabitants/year for women and 52 for men, rough rate 99/100,000/year (Stevens et al. Neurology 1988; 38:134-8). A study carried out in the Sienese area from 1991 to 1997 (Mondelli M. et al. Toscana Medica July/August 1999) gives a rough rate of incidence of 326.2/100,000/year (135.1 for males and 506.9 for women), the standard incidence being 276.6/100,000/year. The average F: M incidence ratio is 3.8:1. The decade most represented for both sexes is that between 50 and 59 years. The incidence of Carpal Tunnel Syndrome (CTS) is three times higher in women and varies according to the work activities (up to 60 cases for every 100 workers in a particular job): in about 70% of the cases, it is bilateral and is prevalent in the dominant hand.
Is diagnosis of CTS easy?
When the patient complains of tingling (paresthesias) and/or pain, often radiating to the forearm, mainly at night or early in the morning, the condition is most probably due to Carpal Tunnel Syndrome. However, it is necessary to carry out an objective neurological test and EMG/ENG (electromyography/electroneurography) tests.
The objective neurological test examines the strength, the osteotendonitic reflexes, and sensitivity, and can involve clinical tests.
The most common tests are the Tinel and Phalen tests. In the first case, the carpal tunnel is tapped with a reflex hammer and the patient must feel a shock in the median nerve distribution area; the second test consists in bending or stretching the hand over the forearm for one minute; the patient must feel a tingling sensation or the tingling sensation must worsen.
However, the tests can often give negative false or positive false results; it is therefore not advisable to rely too much on the results obtained. Therefore an EMG/ENG test is recommended.
The ENG (electroneurographic) test involves the use of surface electrodes for sending small electric shocks and makes it possible to test the sensation speed (the first factor that is affected in the Carpal Tunnel Syndrome) the motorial speed, the latency and amplitude of sensory and motor responses of the nerve felicitated by the electric shock. However, to estimate the severity of the syndrome and exclude nervous problems at different levels (for example, cervical compression), the tests must be completed with the EMG test, using tiny needles to record the muscular activity.
Cervical radiculopathy, brachial plexus problems, and polyneuropathy in general often give rise to symptoms that simulate the Carpal Tunnel Syndrome, and only a correct complete test will help detect the difference.
The latter also allows classification of the extent of the damage.
In some patients, even the first stage of the problem, with negative EMG/ENG result can still be very troublesome. Diagnosis of Carpal Tunnel Syndrome is therefore usually not very difficult if the diagnostic procedure is complete.
What is the evolution of CTS?
Usually, without treatment or change of job, Carpal Tunnel Syndrome tends to worsen over the years. However, some patients remain stationary in time.
Clinical experience has shown that during cold spells the symptomatology exacerbates and improves during warm spells without modifying the seriousness of the pathology.
Carpal tunnel syndrome treatment
Carpal Tunnel Syndrome therapy can be conservative or chirurgical. According to indications of The American Academy of Neurology (AAN, 1993) conservative treatment is to be tempted if there is no deficit of strength or sensibility or severe anomalies in EMG/ENG tests. It is important, however not to operate on the patient too late, in as much as results may be permanent. Patients in conservative therapy must be checked on.
Conservative sometimes it is sufficient to change one’s working ways to achieve an improvement. To avail with: ultrasound, ionophoresis, laser, that can improve the symptoms but do not act on the cause of the syndrome (repetitive and prolonged wrist flexion/extension): non-steroid anti-inflammatory drugs have scarce effect, steroid drugs have a limited efficiency in time: efficient infiltrations on the symptoms but with two major “side effects”: proven damage to the fibrotic of the nerve and the risk that the Patient puts off the operation for too long with a permanent outcome. Wrist splints are efficient but not well tolerated, usually used at night only and therefore have no effect on the cause of the syndrome. Policarpal (new bracelet) is new; as it efficiently limits wrist flexion/extension without blocking it and allows normal use of the hand (also thumb opposition) therefore it can be used comfortably day and night directly influencing the cause of the pathology.
Chirurgical. The operation foresees a cut in the transverse carpal ligament (roof of the carpal tunnel) sometimes associated with neurolysis. It can be carried out by traditional or endoscopic technique, local or full anesthetic, with an average convalescence of approximately 20 days, a little less if carried out endoscopically. There are no univocal criteria for the choice of chirurgical method. Convalescence is usually between 2 –4 weeks.
Carpal Tunnel Syndrome – All You Need To Know, Last Update: 12/7/2017

Pingback: How To Reverse Carpal Tunnel Syndrome Naturally - Body Pain Tips
Pingback: Are Carpal Tunnel Syndrome and Repetitive Stress Injury the Same Condition - Body Pain Tips
Pingback: 5 Carpal Tunnel Syndrome Causes and Symptoms - Body Pain Tips
Pingback: What are the Warning Signs of Carpal Tunnel Syndrome - Body Pain Tips
Pingback: 9 Yoga Posture for Carpal Tunnel Syndrome Treatment - Body Pain Tips
Pingback: Surgery for Carpal Tunnel Syndrome - Body Pain Tips
Pingback: 7 Exercises to Help Your Carpal Tunnel Syndrome Symptoms - Body Pain Tips
What’s Taking place i’m new to this, I stumbled upon this I’ve found
It absolutely useful and it has aided me out loads.
I hope to contribute & aid other users like its
aided me. Great job.
Thank you, Ernestine, I will continue to post new articles
Pingback: How to Get Rid of Carpal Tunnel after Pregnancy - Body Pain Tips
Pingback: How To Know If You Have Carpal Tunnel Syndrome? - Body Pain Tips
Pingback: How to Cure Carpal Tunnel Syndrome Naturally - Body Pain Tips
Pingback: How is Carpal Tunnel Treated ? - Body Pain Tips
Pingback: What Causes Pain Between Thumb and Index Finger? - Body Pain Tips
Pingback: Sudden Wrist Pain For No Reason - 7 Possible Causes - Body Pain Tips
Pingback: Carpal Tunnel Symptoms in The Wrist - Body Pain Tips